At birth all babies are obligate nasal breathers. This is because it would be fatal for them in the womb if they inhaled amniotic fluid. However many of them subsequently develop short or long-term nasal obstruction and are forced to breathe through their mouth. For some this is temporary, but for others it develops into a long-term or even permanent open mouth posture.
There is some debate about the reason for the nasal obstruction but I am sure it is primarily related to household allergies. It is very important that mothers make every effort to encourage their child to keep their mouth closed. Many people are unaware that mouth breathing itself increases nasal congestion. So this can become a vicious circle. When I first suggested that lips could be taped, nearly 30 years ago, I was accused of child cruelty or worse. At that time I suggested two vertical strips of non-allergic tape, merely to act as a reminder.
There is much contradiction about how best to open the airway. The traditional treatment has been to remove the tonsils and adenoids which are presumed by many to be the cause. However I was influenced by the work of Brian Preston (1979) who used tomography to show than the upper airway is rarely obstructed by even large tonsils or adenoids. Instead I found that if my Stage 1 appliance was expanded at the semi-rapid rate for ten millimetres the airway would always enlarge enough for normal nasal respiration.
However there is a snag. If the child does not learn to breathe primarily through the nose the nasal airway will block again within eighteen months. This is why expansion must be coupled with training, but in my opinion the removal of tonsils and adenoids is usually unnecessary. Recent research has shown this ring of lymphoid tissue is an important part of the immune system and in any case usually shrinks as the child passes the age of ten.
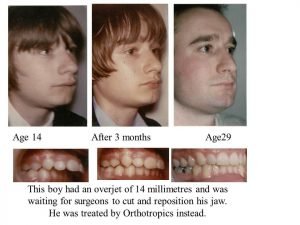
I have no doubt that a lot of long-term facial damage is done in the first three years of open mouth growth. Babies look attractive anyway and it is often not until the pre-pubertal growth spurt at the age of 7 or 8 that the true vertical growth is exposed (see illustration below). Sadly by then it may be too late to restore a natural closed lip posture.


Quite apart from the lip posture, by the age of 8 it is often too late to restore the structural damage that has been done to the maxilla. This is why the majority of children from highly civilised countries are doomed to grow up with flat cheeks and big noses. The sad thing is that this could be avoided if only their parents realized the importance of keeping the mouth closed and I constantly recommend that treatment should start before the age of 8. The influence of an open mouth posture is huge even as late as 10 years old (see picture below).
I have been surprised that the orthodontic specialty has been so slow in recognising this damage. It was not really accepted until 1997 when Trotman, McNamara, Dibbets and Th van der Weele published their seminal paper. Even now I find many orthodontists give little importance to lip training .
If there are any other topics you want us to cover please let us know.
As a general rule neither Prof or Dr Mew have time to engage in the comments section, their focus must be to gain as much real change and scientific engagement as possible, and this would otherwise consume all their time. If you want to engage with Prof John Mew or Dr Mike Mew on this or other topics then follow these links;
Professionals (of any medical/health discipline); https://www.facebook.com/groups/Ortho… or https://www.facebook.com/groups/Ortho…
Non Professionals; https://www.facebook.com/groups/crani… or https://www.facebook.com/groups/crani…
For more general information please visit; https://orthotropics.suryawebsolution.com.np/
Please consider joining our Patreon Community: https://www.patreon.com/orthotropics Particularly if you have; 1) gained any benefit from the information that we have provided (usually for free). 2) wish to have the benefits of being a patreon member. 3) believe in, and wish to support our mission to gain full, free and fair debate (engagement) on these issues within the orthodontic and dental community. Currently the full proceeds of the patreon is directed to the video team, who donate the rest of their time for free. Please help in spreading this message.