Orthotropics 14. Age for treatment.
Precis. What age should parents be advised about the cause of malocclusion and should treatment be started before the growth spurts at seven or twelve? My father was told it should be five I was taught thirteen and my son was taught when the permanent teeth had erupted. Which is correct? Certainly parents deserve sound advice so they can seek treatment at the appropriate time.
Lecture 14, My father who was also an orthodontist told me that when he trained in 1921 he was told to consider orthodontic treatment from the age of four onwards. If at the age of five there was not room for “Half a Crown” (a UK coin about 2mm thick) between each upper incisor, then you should expand. Why have orthodontists changed so much since then?

His teacher at Guys hospital was Harold Chapman who was probably the best known orthodontist in the UK. In 1936 I became a patient of Chapman at the age of 8 when he expanded my narrow jaw. I must now be one of the last of his patients still alive. Out of interest I looked up some of his lectures and found that the ‘correct age of treatment’ was his special interest.
At one meeting in America he said “it seemed to me not inappropriate to promote a new discussion on the age for orthodontic treatment at such a representative gathering as this”.
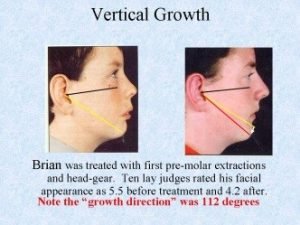
“Translated into practical terms, the reason age is a predominant factor is that at one period early treatment may give good results, and at another, the late period, good results may be an impossibility; in the intermediate period treatment looked at from every point of view gradually degenerate from good to very poor as the age increases”. Not everyone would agree with him today but few could prove him wrong.
Certainly I find expansion under the age of six quite simple and usually children at this age are very compliant. The thing that is difficult is changing their posture. I am sure that it was this last factor that persuaded orthodontists in the 1930s to delay treatment to the start of Puberty. Because if they could not change oral posture their cases quickly relapsed during the deciduous changeover. Therefore it made sense to them to wait until the changeover was complete. However by this age Maxillary change was very difficult.
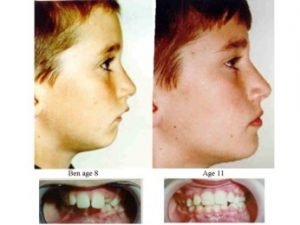
I don’t think I can give a better example than my own son Mike. At the age of five his deciduous incisors were slightly crowded which is a sign that there will be severe crowding in the future. At that time I had not developed the Indicator Line but I could see that his face was growing vertically. So I expanded him at the semi-rapid rate with a Stage 1 Biobloc appliance.

After four months there was plenty of space and you can see the un-erupted central incisors had moved apart showing the central suture had widened. He subsequently had Stage 3 and 4 appliances which gave him an entirely different facial form compared to his father.
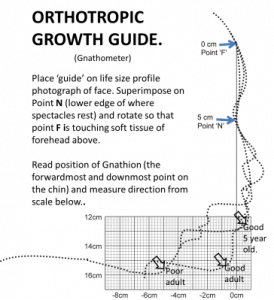
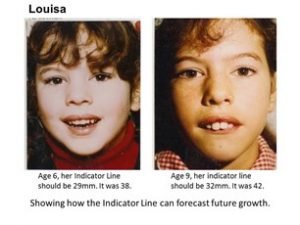
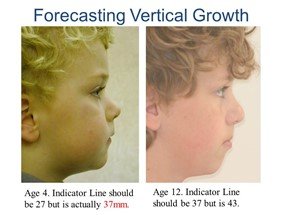
I should add that his mother’s maxilla was narrower than mine. I would recommend that either the Clinician or Parent measures the Indicator line around the age of three or four. If it is increased then efforts should be made to improve mouth posture and possibly commence treatment by five. Failure to do this can have severe consequences.
As a general rule neither Prof or Dr Mew have time to engage in the comments section, their focus must be to gain as much real change and scientific engagement as possible, and this would otherwise consume all their time. If you want to engage with Prof John Mew or Dr Mike Mew on this or other topics then follow these links (if you want a personal opinion on your situation then please book an on-line consultation at https://orthodontichealth.co.uk/book-…
Professionals (of any medical/health discipline); https://www.facebook.com/groups/Ortho… or https://www.facebook.com/groups/Ortho…
Non Professionals; https://www.facebook.com/groups/crani… or https://www.facebook.com/groups/crani…
For more general information please visit; https://orthotropics.suryawebsolution.com.np/
Please consider joining our Patreon Community: https://www.patreon.com/orthotropics Particularly if you have; 1) gained any benefit from the information that we have provided (usually for free). 2) wish to have the benefits of being a patreon member. 3) believe in, and wish to support our mission to gain full, free and fair debate (engagement) on these issues within the orthodontic and dental community.